HealthAuthorityLife Editorial Team | July 31, 2026
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment of any medical condition.
Key Takeaways
- Hair loss affects approximately 50 million men and 30 million women in the United States, making it one of the most common health concerns people search for online.
- There are multiple types of hair loss including androgenetic alopecia, telogen effluvium, alopecia areata, and traction alopecia, each with different causes and treatment approaches.
- Early intervention is critical. Most treatments work best when started early, before significant hair follicle damage occurs.
- FDA-approved treatments including minoxidil (Rogaine) and finasteride (Propecia) have decades of clinical research supporting their effectiveness.
- Natural approaches including nutrition optimization, stress management, and scalp care can complement medical treatments.
- Hair loss can be a symptom of underlying conditions like thyroid dysfunction, iron deficiency, autoimmune disease, or hormonal imbalances that require medical attention.
Understanding Hair Loss: How Common Is It?
Hair loss is one of the most frequently searched health topics on Google, and for good reason. According to the American Academy of Dermatology, approximately 80 million people in the United States experience hereditary hair loss alone. By age 50, about 85% of men have significantly thinning hair, and roughly 50% of women will experience noticeable hair loss during their lifetime.
Despite how common it is, hair loss remains deeply personal and often emotionally distressing. Many people suffer in silence, unsure whether their hair loss is temporary or permanent, preventable or inevitable. The good news is that most forms of hair loss are treatable, especially when addressed early. Understanding the root cause is the first and most important step toward finding an effective solution.
This comprehensive guide covers everything you need to know about the causes of hair loss, the different types you might encounter, the most effective treatments available, and when to seek professional medical help.
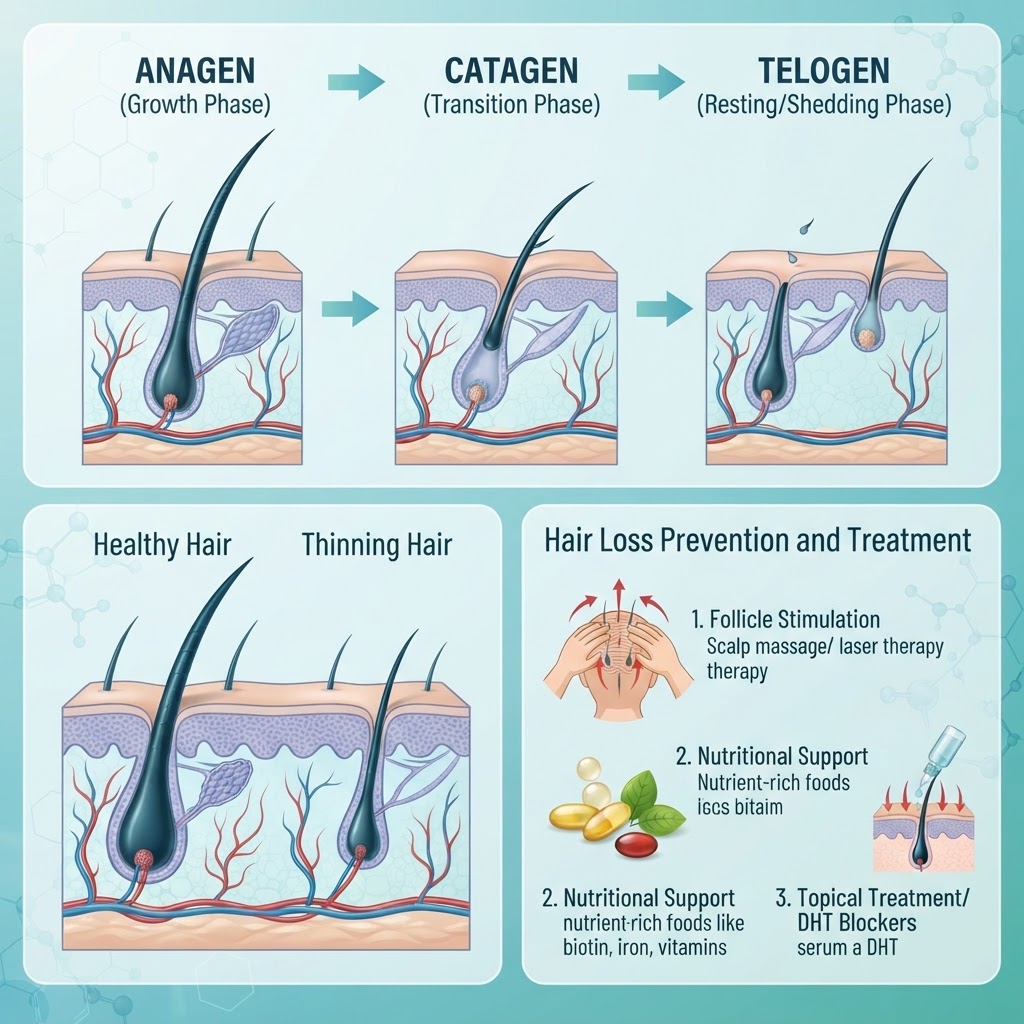
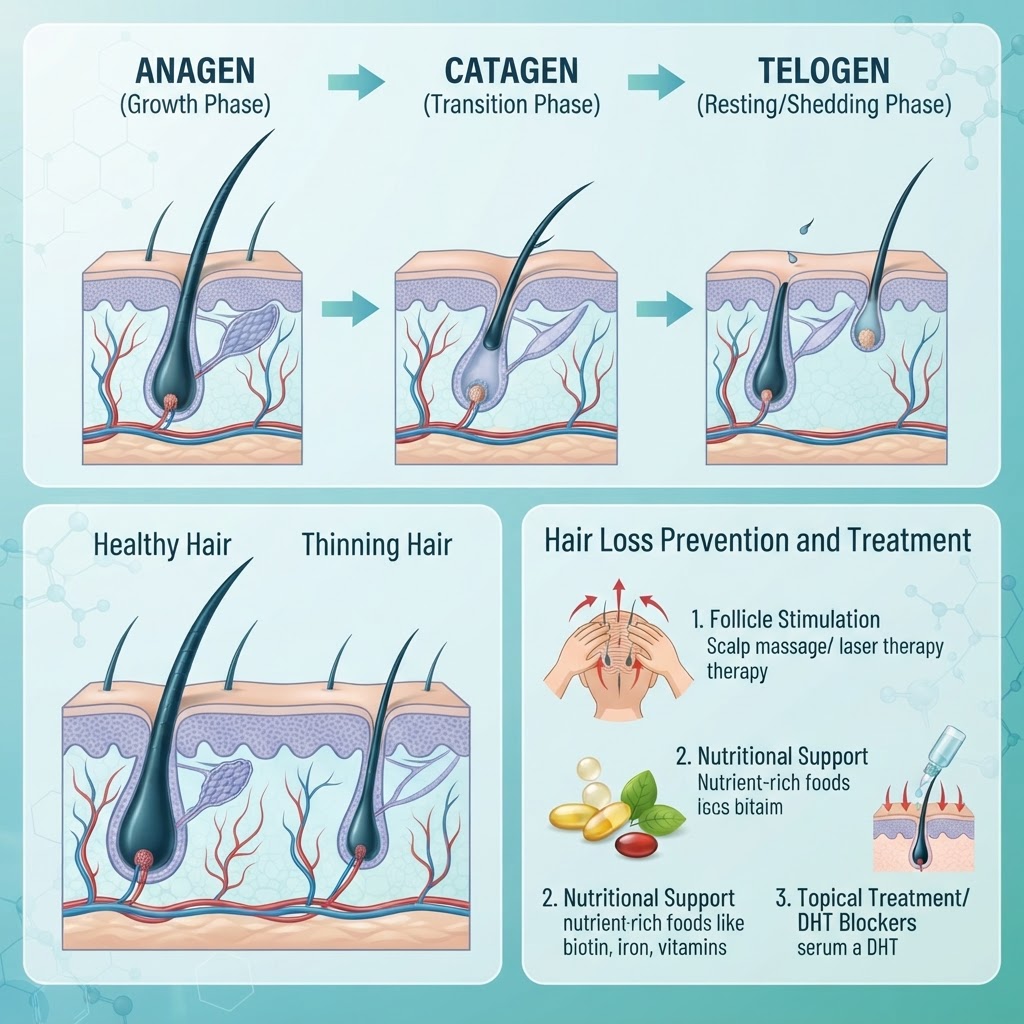
The Hair Growth Cycle: Understanding How Hair Works
To understand hair loss, it helps to first understand how hair grows. The human scalp contains approximately 100,000 hair follicles, and each one goes through a growth cycle consisting of three main phases:
Anagen Phase (Growth Phase)
This is the active growth phase, lasting between 2 to 7 years. During anagen, hair grows approximately 1 centimeter every 28 days. The length of this phase determines how long your hair can grow. About 85 to 90 percent of your hair is in the anagen phase at any given time. When this phase shortens due to genetics, stress, or medical conditions, hair becomes thinner and shorter over time.
Catagen Phase (Transitional Phase)
This is a brief transitional period lasting about 2 to 3 weeks. During catagen, the hair follicle shrinks and detaches from the blood supply. Only about 1 to 2 percent of your hair is in this phase at any time. The hair stops growing but does not yet fall out.
Telogen Phase (Resting and Shedding Phase)
This phase lasts about 3 to 4 months. The hair follicle rests while a new hair begins to form beneath it. At the end of telogen, the old hair falls out and the new hair pushes through the scalp. About 10 to 15 percent of your hair is in this phase normally. Losing 50 to 100 hairs per day is considered normal and is part of this natural cycle.
Hair loss occurs when this cycle is disrupted, when the anagen phase shortens, when too many follicles enter telogen simultaneously, or when new hairs fail to grow after old ones fall out.
Types of Hair Loss: Identifying What You Have
1. Androgenetic Alopecia (Pattern Hair Loss)
This is by far the most common type of hair loss, affecting both men and women. In men, it typically presents as a receding hairline and thinning at the crown, eventually forming a U-shaped pattern. In women, it usually manifests as diffuse thinning across the top of the scalp while the front hairline is generally preserved.
Androgenetic alopecia is hereditary and is driven by the hormone dihydrotestosterone (DHT), a derivative of testosterone. DHT binds to hair follicle receptors, causing them to shrink over successive growth cycles. The follicles produce progressively thinner, shorter hairs until they stop producing hair altogether.
This type of hair loss can begin as early as the late teens or early twenties in men who are genetically predisposed. In women, it often becomes more noticeable after menopause when estrogen levels decline.
2. Telogen Effluvium
This is a temporary form of hair loss that occurs when a large number of hair follicles enter the telogen (resting) phase simultaneously. This can be triggered by:
- Severe stress or emotional trauma
- Major surgery or illness
- Significant weight loss or crash dieting
- Childbirth (postpartum hair loss)
- High fever or severe infection
- Certain medications
- Thyroid imbalances
- Iron deficiency
Telogen effluvium typically occurs 2 to 3 months after the triggering event and can cause dramatic shedding that alarms many people. However, it is usually self-limiting. Once the underlying trigger resolves, hair typically regrows within 6 to 9 months. In chronic cases lasting more than 6 months, medical evaluation is recommended.
3. Alopecia Areata
This is an autoimmune condition in which the immune system attacks hair follicles, causing hair to fall out in round patches. It can affect the scalp, beard, eyebrows, and other body hair. In rare cases, it can cause complete scalp hair loss (alopecia totalis) or complete body hair loss (alopecia universalis).
Alopecia areata affects approximately 6.8 million people in the United States. It can occur at any age but most commonly begins before age 40. The condition is unpredictable. Hair may regrow on its own, fall out again, or persist long-term. Treatment options include corticosteroid injections, topical immunotherapy, and newer JAK inhibitor medications that have shown promising results in clinical trials.
4. Traction Alopecia
This type of hair loss is caused by repeated tension on the hair shafts from tight hairstyles such as braids, ponytails, extensions, and buns. Over time, the constant pulling damages the hair follicles and can lead to permanent hair loss along the hairline and temples.
Traction alopecia is preventable and reversible in its early stages. Wearing looser hairstyles, taking breaks from extensions, and avoiding chemical relaxers can help prevent permanent damage. Once follicles are scarred and destroyed, however, the hair loss becomes permanent and may require hair transplant surgery.
5. Cicatricial (Scarring) Alopecia
This rare form of hair loss occurs when inflammation destroys hair follicles and replaces them with scar tissue. Once scarred, follicles cannot regrow hair. Types include lichen planopilaris and frontal fibrosing alopecia. Treatment focuses on stopping the inflammatory process to prevent further hair loss, though already-lost hair cannot be recovered without transplant.
What Causes Hair Loss? Understanding the Root Factors
Genetics and Family History
Genetics is the single most significant factor in androgenetic alopecia. If your father, mother, or grandparents experienced hair loss, your risk is substantially higher. Genetic testing can identify susceptibility markers, though it is not yet standard clinical practice for diagnosis.
Hormonal Changes
Hormones play a major role in hair growth and loss. Key hormonal triggers include:
- Thyroid dysfunction: Both hypothyroidism and hyperthyroidism can cause hair thinning
- Pregnancy and postpartum: Hormonal shifts can trigger telogen effluvium
- Menopause: Declining estrogen can unmask androgenetic pattern hair loss
- Polycystic ovary syndrome (PCOS): Elevated androgens can cause thinning in women
- Hormonal birth control: Starting or stopping certain contraceptives can trigger shedding
Nutritional Deficiencies
Several nutrient deficiencies are strongly linked to hair loss:
- Iron: The most common nutritional deficiency linked to hair loss, especially in women
- Vitamin D: Low levels are associated with both telogen effluvium and alopecia areata
- Zinc: Essential for hair follicle function and tissue repair
- B vitamins (especially biotin): Important for hair structure, though deficiency is rare
- Protein: Hair is primarily made of protein (keratin), and insufficient intake can cause thinning
- Selenium: Both deficiency and excess can trigger hair loss
Stress
Both acute and chronic stress can contribute to hair loss through multiple mechanisms. Severe stress can trigger telogen effluvium by pushing large numbers of follicles into the resting phase. Chronic stress also elevates cortisol, which can interfere with hair follicle cycling and contribute to inflammation.
Medications
Many medications can cause hair loss as a side effect, including:
- Blood thinners (anticoagulants)
- Beta-blockers and ACE inhibitors
- Antidepressants and mood stabilizers
- Retinoids (vitamin A derivatives)
- Chemotherapy drugs
- Non-steroidal anti-inflammatory drugs (NSAIDs) in high doses
If you suspect a medication is causing hair loss, do not stop taking it without consulting your doctor. They may be able to switch you to an alternative.
Medical Conditions
Hair loss can be a symptom of underlying medical conditions including thyroid disease, lupus, diabetes, iron-deficiency anemia, and scalp infections like ringworm (tinea capitis). Identifying and treating the underlying condition often resolves the hair loss.
FDA-Approved Medical Treatments for Hair Loss
Minoxidil (Rogaine)
Minoxidil is the most widely used FDA-approved treatment for both male and female pattern hair loss. Originally developed as an oral blood pressure medication, its hair growth side effect led to its reformulation as a topical solution or foam. It is available over the counter in 2% and 5% strengths.
Minoxidil works by increasing blood flow to hair follicles and extending the anagen (growth) phase. It is most effective on the crown and top of the scalp. Results typically become visible after 3 to 6 months of consistent use. If treatment is stopped, any hair regrown will be lost within a few months.
Side effects are generally mild and include scalp irritation, dryness, and unwanted facial hair growth. A less common but notable side effect is initial increased shedding during the first 2 to 8 weeks, which is temporary and actually a sign the medication is working.
Finasteride (Propecia)
Finasteride is an FDA-approved oral prescription medication for male pattern hair loss. It works by inhibiting the enzyme 5-alpha-reductase, which converts testosterone to DHT. By reducing DHT levels, finasteride slows hair loss and can promote regrowth in many men.
Clinical studies show that finasteride stops hair loss in approximately 86% of men and produces visible regrowth in about 65% of men after two years of treatment. It is most effective when started early in the hair loss process.
Side effects occur in approximately 1 to 2% of men and may include decreased libido, erectile dysfunction, and reduced ejaculate volume. These effects typically resolve after discontinuation. Women who are pregnant or may become pregnant should never handle crushed or broken finasteride tablets due to risk of birth defects.
Dutasteride
Though not specifically FDA-approved for hair loss (it is approved for enlarged prostate), dutasteride is similar to finasteride but blocks both types of 5-alpha-reductase. Some studies suggest it may be more effective than finasteride, though it is used off-label for hair loss.
Low-Level Laser Therapy (LLLT)
LLLT uses red light therapy to stimulate hair follicles. FDA-cleared devices include laser combs, caps, and helmets. Studies suggest it can improve hair density and thickness, particularly when used in combination with minoxidil or finasteride. It is painless, has no known side effects, and can be used at home.
Emerging and Advanced Treatments
Platelet-Rich Plasma (PRP) Therapy
PRP therapy involves drawing your blood, separating the platelet-rich plasma, and injecting it into the scalp at areas of hair loss. Platelets contain growth factors that may stimulate hair follicle activity. Several studies have shown promising results, though more large-scale research is needed. Treatment typically requires multiple sessions spaced a month apart, with maintenance sessions every 6 months.
Hair Transplant Surgery
For permanent hair loss where follicles are no longer functional, hair transplant surgery can relocate healthy follicles from the back and sides of the scalp to thinning areas. Modern techniques include Follicular Unit Extraction (FUE) and Follicular Unit Transplantation (FUT). Results are permanent because the transplanted follicles are genetically resistant to DHT.
JAK Inhibitors
A newer class of medications called JAK inhibitors (such as baricitinib and ruxolitinib) has shown remarkable results for alopecia areata. The FDA approved baricitinib for severe alopecia areata in 2022, making it the first systemic treatment specifically approved for this condition.
Natural and Lifestyle Approaches to Support Hair Health
Nutrition for Healthy Hair
A balanced diet rich in the following nutrients can support healthy hair growth:
- Protein: Eggs, fish, lean meats, beans, and lentils provide the amino acids needed for keratin production
- Iron: Red meat, spinach, lentils, and fortified cereals help prevent iron-deficiency-related hair loss
- Vitamin C: Citrus fruits, bell peppers, and strawberries enhance iron absorption and support collagen production
- Zinc: Oysters, pumpkin seeds, and chickpeas support follicle function
- Vitamin D: Fatty fish, fortified dairy, and safe sun exposure
- Biotin: Eggs, nuts, seeds, and sweet potatoes
- Omega-3 fatty acids: Salmon, walnuts, and flaxseeds reduce inflammation
Scalp Care
A healthy scalp environment supports healthy hair growth. Regular gentle washing, avoiding harsh chemicals, and using a sulfate-free shampoo can help maintain scalp health. Scalp massage may increase blood circulation and has been shown in small studies to increase hair thickness.
Stress Management
Since stress is a known trigger for telogen effluvium, managing stress through regular exercise, meditation, adequate sleep, and relaxation techniques can support hair health. Reducing chronic stress may help prevent stress-related shedding and support overall hair regrowth.
Avoid Damaging Practices
Limit the use of heat styling tools, chemical treatments (perms, relaxers, bleaching), and tight hairstyles. These can damage the hair shaft and, in the case of traction alopecia, permanently damage follicles.
Hair Loss in Women: Special Considerations
Female hair loss often differs from male hair loss in pattern, causes, and treatment. Women are more likely to experience diffuse thinning rather than receding hairlines. Common causes in women include hormonal changes (pregnancy, menopause, PCOS), iron deficiency, thyroid dysfunction, and stress.
Women should not use finasteride due to potential birth defects. Minoxidil 2% is FDA-approved for women, while the 5% formulation is also commonly prescribed. Birth control pills may help regulate hormones in women with PCOS-related hair loss. Spironolactone, an anti-androgen medication, is sometimes prescribed off-label for female pattern hair loss.
Female hair loss can be particularly distressing due to societal expectations around hair and femininity. Support groups and counseling can be valuable resources for women experiencing significant hair loss.
When to See a Doctor About Hair Loss
While some hair loss is normal, certain signs warrant professional medical evaluation:
- Sudden or rapid hair loss that occurs over a few weeks
- Patchy hair loss with smooth, bare areas
- Hair loss accompanied by itching, burning, redness, scaling, or pain on the scalp
- Hair loss with other symptoms like fatigue, weight changes, or mood changes (possible thyroid or other systemic condition)
- Hair loss that persists beyond 6 months despite addressing obvious triggers
- Hair loss causing significant emotional distress
- Any signs of infection such as pus or open sores
A dermatologist can diagnose the type of hair loss through physical examination, scalp biopsy, blood tests, or pull tests. Early diagnosis and treatment generally produces better outcomes.
Frequently Asked Questions
Can stress really cause hair loss?
Yes. Severe or prolonged stress can trigger telogen effluvium, a condition where a large number of hair follicles enter the resting phase simultaneously. This typically causes noticeable shedding 2 to 3 months after the stressful event. Stress-related hair loss is usually temporary and resolves once the stress is managed.
Does wearing a hat cause hair loss?
No, wearing a hat does not cause hair loss. This is a common myth. Hair loss occurs at the follicle level beneath the scalp, and a hat cannot affect follicle function. However, very tight hats worn constantly could potentially cause mild traction, though this is rare.
How long does it take for hair loss treatments to work?
Most treatments require at least 3 to 6 months of consistent use before visible results appear. Hair grows slowly, about 1 centimeter per month, so patience is essential. Stopping treatment prematurely is the most common reason for perceived treatment failure.
Is hair loss reversible?
It depends on the cause. Telogen effluvium is usually fully reversible. Alopecia areata can be temporary or recurring. Androgenetic alopecia is progressive but can be slowed significantly with treatment. Scarring alopecias cause permanent loss. The earlier treatment begins, the better the outcome.
Can diet alone reverse hair loss?
If your hair loss is caused by a nutritional deficiency, correcting the deficiency through diet or supplements can restore hair growth. However, genetic and hormonal hair loss requires medical treatment. Diet supports hair health but cannot overcome genetic pattern hair loss on its own.
Are hair loss supplements effective?
Supplements can help if you have a specific deficiency. However, many marketed hair supplements contain ingredients that have limited evidence of effectiveness. Biotin supplements, for example, only help if you are actually deficient, which is rare. Consult a doctor before starting supplements.
Does insurance cover hair loss treatment?
Most insurance plans do not cover treatments for androgenetic alopecia, considering it cosmetic. However, if hair loss is caused by a medical condition like thyroid disease or lupus, treatment for the underlying condition is typically covered. PRP therapy and hair transplants are usually out-of-pocket expenses.
Conclusion: Taking Action Against Hair Loss
Hair loss is a common but treatable condition. The key is understanding the cause, seeking professional diagnosis early, and committing to a consistent treatment plan. Whether your hair loss is genetic, stress-related, nutritional, or medical, there are more treatment options available today than ever before.
Remember that hair loss is a medical issue, not a vanity concern. If you are experiencing hair loss, consult a dermatologist or your healthcare provider. They can determine the cause and recommend the most appropriate treatment plan for your specific situation.
This article was written by the HealthAuthorityLife Editorial Team and reviewed for medical accuracy. Last updated July 2026.
Hair Loss Myths vs Facts: What the Science Actually Says
Hair loss is surrounded by myths that can lead people to waste money on ineffective treatments or neglect actual medical issues. Understanding the difference between fact and fiction helps you make informed decisions about your hair health.
Myth: Washing Your Hair Every Day Causes Hair Loss
Fact: Washing your hair frequently does not cause hair loss. The hairs that fall out during washing were already in the telogen (shedding) phase and would have fallen out regardless. Using a gentle, sulfate-free shampoo can help maintain scalp health without causing damage.
Myth: Brushing Your Hair 100 Strokes a Day Promotes Growth
Fact: Excessive brushing can actually cause breakage and damage the hair shaft. While gentle brushing helps distribute natural oils through the hair, aggressive brushing does not stimulate growth and may cause more harm than good.
Myth: Hair Loss Only Comes From Your Mothers Side
Fact: The genetics of hair loss are complex and involve genes from both parents. While the androgen receptor gene is on the X chromosome (inherited from the mother), multiple other genes from both sides contribute to hair loss susceptibility. Blaming only your maternal grandfather oversimplifies the genetics.
Myth: Stress Causes Permanent Hair Loss
Fact: Stress-related hair loss (telogen effluvium) is typically temporary. Once the stressor is removed or managed, hair usually regrows within 6 to 9 months. However, chronic stress can exacerbate other forms of hair loss, so stress management remains important for overall hair health.
Myth: Hair Loss Means You Have a Serious Health Problem
Fact: The most common form of hair loss (androgenetic alopecia) is benign and not associated with any health problems. However, sudden or unusual hair loss can signal underlying conditions, which is why medical evaluation is recommended for new or rapidly progressing hair loss.
The Psychological Impact of Hair Loss
Hair loss is not just a cosmetic concern. Studies have shown that it can significantly impact mental health and quality of life. A study published in the Journal of the American Academy of Dermatology found that hair loss can lead to anxiety, depression, reduced self-esteem, and social withdrawal in both men and women.
The psychological impact is often disproportionate to the physical severity. Some people with minor hair loss experience significant distress, while others with extensive loss are relatively unaffected. This variability highlights the importance of addressing the emotional aspects of hair loss alongside the physical treatment.
If hair loss is affecting your mental health, consider speaking with a therapist or counselor. Support groups, both in-person and online, can also provide valuable emotional support from others experiencing similar challenges. Treating the psychological impact is just as important as treating the hair loss itself.
Hair Loss Treatments on the Horizon: What Is Coming Next
The field of hair loss treatment is rapidly advancing. Several promising approaches are in various stages of research and clinical trials:
Stem Cell Therapy
Researchers are exploring ways to use stem cells to regenerate hair follicles. Early studies have shown promise, with some patients seeing new hair growth from stem cell treatments. While not yet FDA-approved, clinical trials are ongoing and results are encouraging.
Hair Cloning
Hair cloning (or hair multiplication) involves taking a small number of hair follicle cells, multiplying them in a laboratory, and injecting them back into the scalp to create new follicles. This approach could potentially provide unlimited hair for transplantation. While still in experimental stages, it represents one of the most exciting possibilities in hair loss research.
JAK Inhibitors for Androgenetic Alopecia
While currently approved for alopecia areata, JAK inhibitors are being studied for their potential in treating androgenetic alopecia as well. Early research suggests they may help reactivate dormant follicles.
Topical Anti-Androgens
Researchers are developing topical treatments that block DHT locally at the scalp without systemic side effects. This could provide an alternative to oral finasteride for those concerned about side effects.
3D-Printed Hair Follicles
Scientists at Columbia University have successfully grown human hair follicles in 3D-printed molds. This technology, while years away from clinical use, could eventually provide a limitless source of hair follicles for transplantation.
Hair Loss in Different Populations: Age, Gender, and Ethnicity Considerations
Hair Loss in Young Adults
Hair loss in people under 25 is more common than many realize. Approximately 25% of men with androgenetic alopecia begin seeing signs before age 21. For young adults, early intervention is especially important because treatments are more effective when started before significant follicle damage occurs. Young people experiencing hair loss should see a dermatologist promptly rather than waiting.
Hair Loss in Older Adults
Hair thinning accelerates with age as hair follicles naturally become less active and the anagen phase shortens. By age 70, nearly all people experience some degree of hair thinning. In older adults, it is important to distinguish between age-related changes and treatable conditions like thyroid dysfunction or medication side effects.
Ethnic Differences in Hair Loss
Hair loss patterns and prevalence vary across ethnic groups. Androgenetic alopecia is most common in Caucasian men, less common in Asian men, and least common in Native American men. Women of all ethnicities experience pattern hair loss, though the patterns and severity may differ. Traction alopecia is more common in populations where tight braiding and hair extensions are culturally prevalent. Understanding these differences helps ensure appropriate diagnosis and treatment for all patients.
Building a Hair Care Routine That Supports Growth
While no hair care routine can cure genetic hair loss, a healthy scalp environment supports the effectiveness of medical treatments. Here are evidence-based recommendations:
- Wash regularly: Clean scalp supports healthy follicles. Wash every 1-3 days depending on hair type and scalp oiliness.
- Use gentle products: Sulfate-free shampoos and silicone-free conditioners are gentler on hair and scalp.
- Avoid excessive heat: Limit blow drying, flat ironing, and curling to prevent damage to the hair shaft.
- Massage your scalp: A 2016 study found that 4 minutes of daily scalp massage increased hair thickness over 24 weeks.
- Protect from sun: UV damage affects scalp skin. Wear a hat in intense sun or use SPF on exposed scalp areas.
- Be patient: Hair grows slowly. Any treatment or routine needs 3-6 months minimum to show results.
Hair Loss Supplements: What Works and What Is Marketing
The supplement industry markets numerous products for hair loss, but evidence varies dramatically. Here is what the research supports:
Supplements With Some Evidence
- Iron: If you have a documented iron deficiency (confirmed by blood test), iron supplementation can restore hair growth. Do not supplement iron without testing, as excess iron can cause health problems.
- Vitamin D: Low vitamin D levels are linked to hair loss. If you are deficient, supplementation may help. Most people can benefit from 1,000-2,000 IU daily, but confirm with your doctor.
- Zinc: Zinc deficiency can cause hair loss. Supplementing helps if you are deficient, but excessive zinc can cause copper deficiency and other issues.
Supplements With Limited Evidence
- Biotin: Despite being in nearly every hair supplement, biotin only helps if you are actually deficient, which is rare. High-dose biotin can interfere with lab test results, including thyroid tests and cardiac markers.
- Saw Palmetto: Some small studies suggest it may have mild DHT-blocking effects, but evidence is insufficient to recommend it as a treatment.
- Marine collagen: Preliminary studies suggest possible benefits for hair thickness, but large-scale studies are lacking.
Supplements to Avoid or Question
- High-dose vitamin A: Excess vitamin A actually causes hair loss. Do not exceed recommended daily amounts.
- Selenium in high doses: Both deficiency and excess of selenium can cause hair loss. More is not better.
- Multi-ingredient hair formulas: Many contain sub-therapeutic doses of everything, making them expensive but potentially ineffective. Targeted supplementation based on your specific deficiency is more effective.
Always consult your doctor before starting any supplement regimen. Blood tests can identify actual deficiencies, making targeted supplementation more effective and safer than taking a shotgun approach.

